 23.45°C Kathmandu
23.45°C Kathmandu

Thu, Jun 18, 2026
Miscellaneous
Ebola in Nepal
During my recent personal visit to the country, I had the opportunity to observe Nepal’s level of preparedness against a possible
bookmarkDuring my recent personal visit to the country, I had the opportunity to observe Nepal’s level of preparedness against a possible outbreak of the Ebola Virus Disease. I was struck by how inadequately Nepal is prepared to handle possible cases of Ebola and to prevent its outbreak.
Dr Sanjeeb Sapkota
Published at : January 23, 2015
Updated at : January 24, 2015 09:00
While I observed some impressive work to manage Ebola here: there is a voluntary reporting desk at the airport immigration; we have a point person in the Ministry of Health and the Nepal office of the World Health Organization; the temperatures of the returning peacekeepers are checked and they are confined to a mandatory quarantine. But I observed that much more would need to be in place if a possible outbreak were to be managed.
Nepal was much better prepared during the pre-pandemic influenza period, in 2008, when the fear of bird flu outbreak with H5N1 was at its height. I had thought similar preparedness measures would have been in place for Ebola, but I found only a fraction of the response measures that Nepal had instituted for bird flu.
The lack of preparedness for Ebola could be due to a number of reasons. Ebola is still viewed by some countries as a regional problem isolated to West Africa. It has not yet manifested as a global disease. The absence of Ebola cases so far in South Asia (except for a few suspected cases) has meant that heightened concern has not been triggered. Ebola is not yet a priority as pandemic influenza was back in 2008. The lack of resources, budget and skilled individuals to handle the cases could be another reason that Ebola is not a priority.
What is mostly lacking regarding Ebola prepraredness is a coordinated national team or central command system comprising the government, non-government organisations, hospitals and all possible stakeholders, just like there was one for the pandemic influenza a few years ago. Such a national team would be able to perform a series of actions such as maintaining an emergency operation centre, conducting regular meetings among the team members to discuss strengths and limitations, identifying resources and gaps and quickly filling them.
Ebola is a disease caused by a virus that has a fatality rate of 50-90 percent. This means that up to 90 out of 100 people who are infected with the disease die from it. The process of death is dreadful. First, the person has flu-like symptoms, followed by diarrhoea, internal and external haemorrhaging, organ failure and eventually, death. So far, as of Jan 19 this year, Ebola has infected more than 21,000 people, mostly in Sierra Leone, Liberia and Guinea. But there have been some cases in Europe and the United States as well. Of those infected with the disease, more than 8,000 have died.
As we have seen in the United States, Europe and Africa, not all hospitals can handle individuals who have the disease. There are few hospitals that are designated as Ebola Treatment Centres (ETC), with the equipment, resources and expertise to manage patients with Ebola. In the United States, hospitals in three places, Atlanta, Nebraska and Bethesda, have been designated as treatment centres, where sick individuals are flown in for treatment. In a similar way, a few centres, call them reference hospitals, should be prepared in Nepal and these hospitals need to be given the equipment and resources to get them ready to receive sick individuals.
Besides these reference hospitals, many other hospitals in all the regions of country should be prepared to provide initial treatment to individuals with Ebola, without the staff’s breaching any safety protocol.
Hospital staff also need to be provided with training on how to handle Ebola cases. And these hospitals should run simulations or drills with dummy patients to practice how to move patients from one place to another without breaching safety measures—from the time of the patients’ arrival to the point of their discharge.
In the United States, one mistaken assumption was that should the disease make landfall in the country, most of the hospitals across the country would be able to handle Ebola cases. This was proven wrong when the first case was diagnosed there. Health personnel working in a Dallas hospital made several errors, both in identifying the case and in providing proper safety measures to prevent contamination. Another mistaken assumption was that the protocols that were prepared and circulated to hospitals would be properly followed by all hospital staff. They were not. The hospitals should have run drills to prepare their staff, to understand where they fell short and where they excelled.
The people too need to be informed. Public awareness of how Ebola is transmitted, how it is not transmitted, what measures are there to prevent it and control it should be circulated widely in simple, culturally appropriate language via radio, television and through flyers placed in schools and public places.
When I was in Nepal, I was invited by Norvic Hospital to share my views on the management of Ebola. During the visit, I got to know firsthand how prepared the hospitals here are. Talking to the staff, I reckoned that to prevent an outbreak occurring on account of an infected person’s landing in the hospital, a lot of training would be needed for the nurses, doctors and paramedics.
I was particularly struck by a question that I was asked: “Can we decline treating an Ebola patient on the grounds that the hospital lacks capacity?” This shows that the hospital staff need to be trained on the ethical aspects of disease too: the protocols to be followed if the hospital lacks the capacity for treating patients.
Being ready for an impending outbreak goes a long way in breaking the transmission of infection, reducing its burden, saving lives and reducing costs for individuals and the nation. This is as true for Ebola as it was for pandemic influenza.
Dr Sanjeeb Sapkota is a medical epidemiologist who works for a government public health agency in the United States. He can be reached at [email protected]





Editor's Picks

Inside the mission of Everest’s first mountain rangers

Weak arbitration defence costs government billions

Nepalis making treacherous trip to Europe through the Balkan route

Women are often at the centre of Nepali films. Why are men still telling most of their stories?
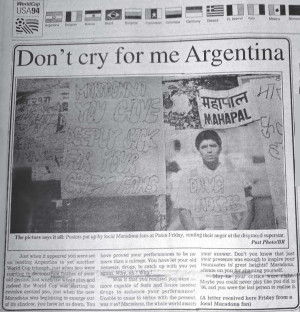
What old newspapers reveal about Kathmandu’s World Cup fever in the 80s and 90s
E-PAPER | June 18, 2026
×